Introduction
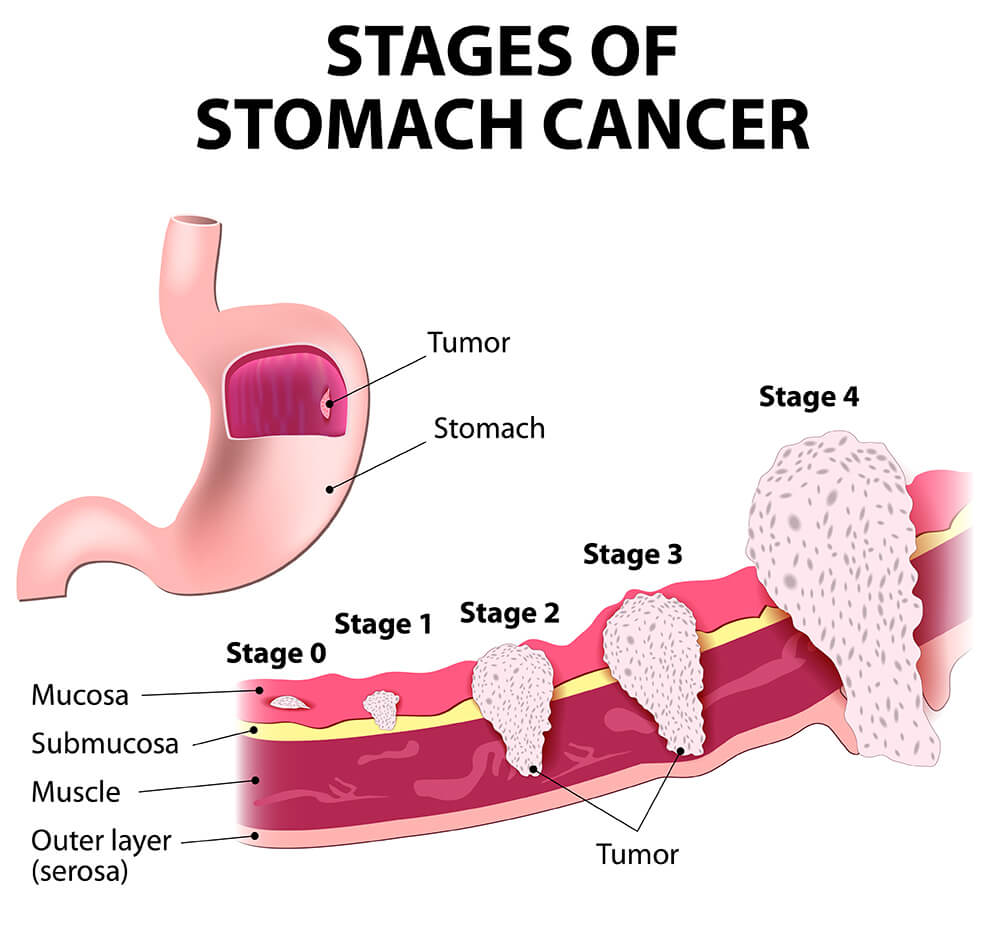
The stomach begins at the gastro-esophageal junction and ends at the duodenum. Cancer cells can grow on the gastric mucosa and spread to adjacent tissue and other parts of the body, causing local and systemic undesirable effects or even death. Gastric cancer is the third most common cause of cancer-related death worldwide and remains difficult to cure in Western countries, primarily because most patients present with advanced disease. Stomach cancer was the sixth commonest cancer in Hong Kong in 2016, accounting for 3.9% of all new cancer cases.
Incidence
There were 1314 new cases of stomach cancer in 2017, with 762 cases in males and 552 cases in females. The male to female ratio was about 1.4 to 1. The crude incidence rates were 22.5 for males and 13.8 for females per 100,000 population of the respective sex. The age-standardised incidence rates were 11.6 for males and 7.3 for females per 100,000 standard population.
Trend of Incidence
The age-standardised incidence rate for both sexes had a downward trend between 1983 and 2016.
Cause / Risk Factors
- Over 40 years of age
- Male to Female ration ~2:1
- Smoking and Alcohol drinking
- Eating salty or pickled foods
- Hereditary or Genetic mutation causes
- Helicobactor infection
- Anemia due to vitamin B12
- People who have prior stomach surgery
- People with rare stomach problems such as gastric acid deficiency
Signs and symptoms
Gastric cancer can present with a variety of signs and symptoms, including:
- Indigestion
- Peptic ulcer pain
- Nausea or vomiting
- Dysphagia (difficulty swallowing)
- Postprandial fullness (feeling full after eating)
- Loss of appetite
- Melena (black feces)
- Pallor from anemia
- Hematemesis (vomiting blood)
- Weight loss and weakness
- Palpable enlarged stomach tumor or swelling
- Succussion splash (a sloshing sound heard during abdominal examination)
- Enlarged lymph nodes, such as:
- Virchow nodes (left supraclavicular area)
- Irish node (anterior axillary area)
Late complications of gastric cancers
Late Complications of Gastric Cancer
As gastric cancer progresses, it may lead to several serious complications:
- Metastatic peritoneal and pleural effusions
- Obstruction of the gastric outlet, gastroesophageal junction, or small bowel
- Bleeding in the stomach from esophageal varices or at the anastomosis after surgery
- Biliary obstruction and jaundice
- Body wasting from starvation or cachexia of tumor origin
診斷
Gastroscopy (or oesophago-gastro-duodenoscopy) with tumor tissue biopsies can confirm the diagnosis of gastric cancer. If gastric cancer is diagnosed by gastroenterologists/gastroenterology physicians, patients with newly diagnosed gastric cancer will be referred to general surgeons for further opinion and treatment.
Role of General Surgeons
General surgeons are the key specialists in managing patients with gastric cancers. They oversee patients through various stages of care:
- Pre-operative stage
- Operative stage
- Post-operative hospital stage
- Follow-up clinic visit stage
Even in advanced or complicated cases, general surgeons contribute to patients' well-being through interventions such as feeding tube placement, endoscopic stenting of obstructing tumors, and providing palliative care.
Role of Clinical Oncologists
Clinical oncologists offer opinions and treatments for:
- Preoperative (neoadjuvant) chemo-irradiation
- Postoperative (adjuvant) chemo-irradiation
- Targeted therapy
They also provide palliative treatment for advanced gastric cancers.
Imaging Studies
Several imaging studies are used to evaluate gastric cancer:
- Chest X-ray (CXR)
- X-ray contrast study
- Ultrasound scan
- CT scan
- MRI scan
- PET CT scan
- PET MR scan
Blood Tests
Gastric cancer tumor markers include CEA and CA 19-9:
- Elevated CEA in 45-50% of cases
- Elevated CA 19-9 in about 20% of cases
Preoperative Staging
After reviewing all the information about the patient and the tumor status, general surgeons will decide the best surgical or non-surgical options for gastric cancer patients.

Surgery
Curative Surgery for Gastric Cancer
The surgical approach in gastric cancer depends on tumor characteristics such as location, size, local invasion, lymph node metastasis, and distant organ or peritoneal metastasis.
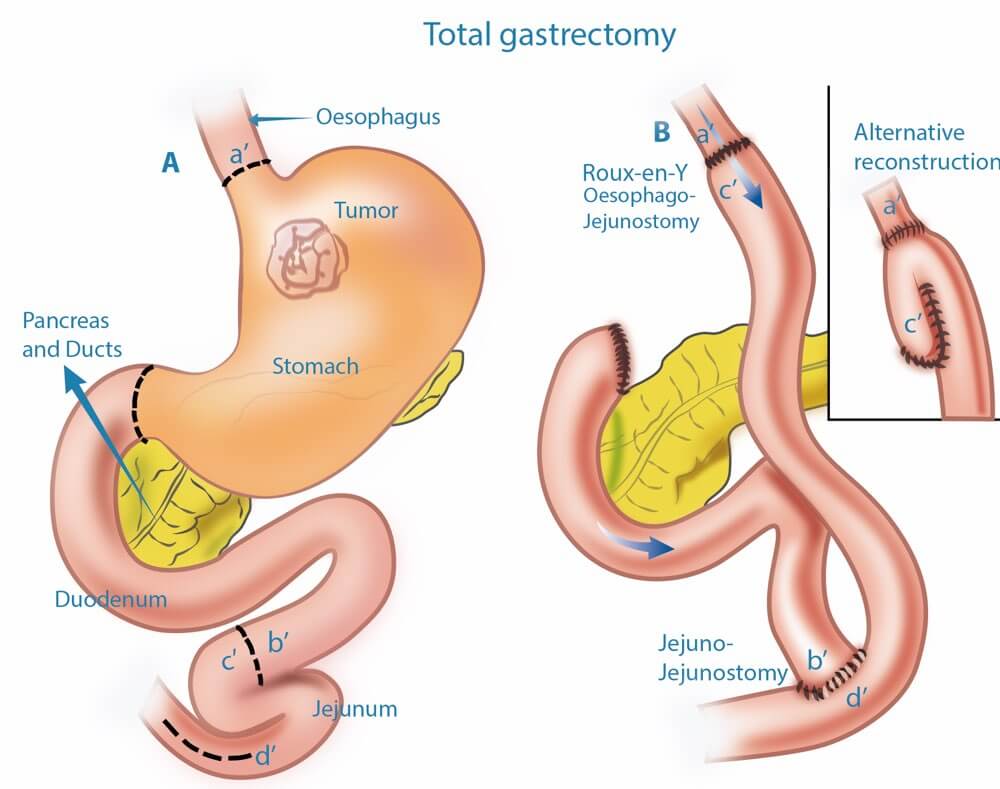
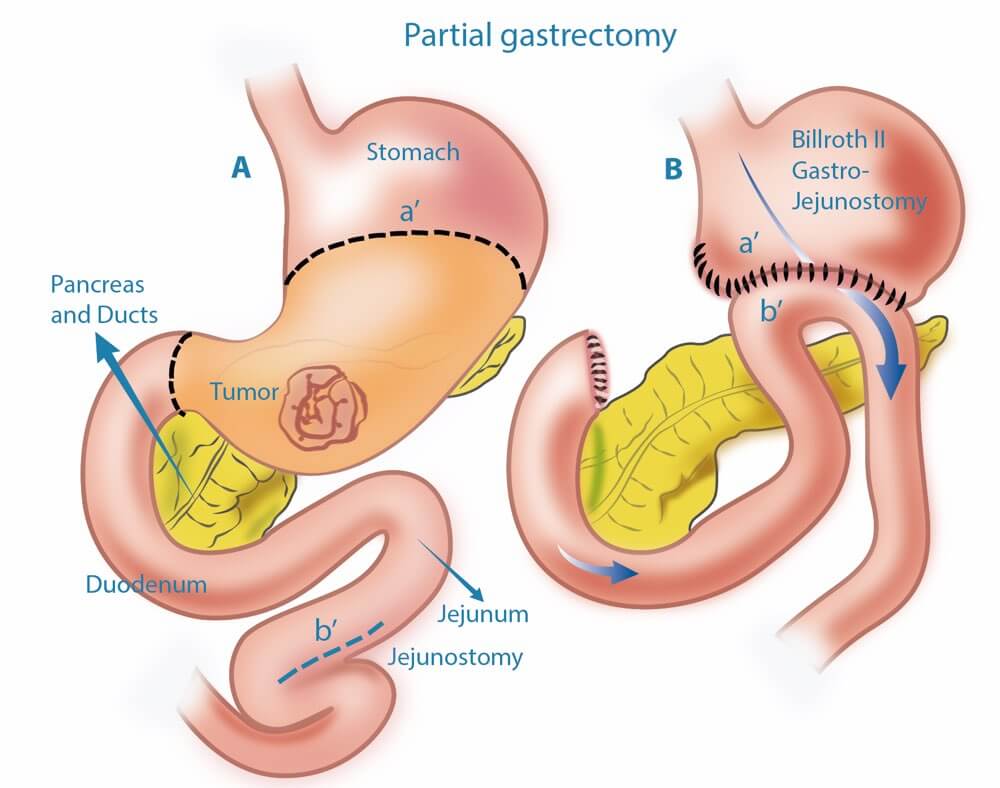
1. Gastrectomy
Gastrectomy is the main treatment for most gastric cancer patients:
- Total Gastrectomy: If the gastric cancer is large, the whole stomach will be excised.
- Partial Gastrectomy: If the gastric cancer is small, part of the stomach will be excised.
General surgeons perform partial or total gastrectomy, which is proven to be the most effective method to treat gastric cancer patients. For early gastric cancer patients, partial or total gastrectomy with surrounding lymph node excisions, along with gastro-intestinal or esophago-intestinal anastomosis, are common operative strategies. Patients can resume eating a few days after surgery. If the cancer has metastasized, general surgeons will weigh the pros and cons of surgical versus non-surgical treatments, considering the patient's wishes to decide the most suitable treatment.
2. Adjuvant Chemotherapy +/- Irradiation Therapy
Chemotherapy and/or irradiation therapy are sometimes used before or after surgery to improve surgical outcomes.
3. Palliative Medicine
If gastric cancer has metastasized, medications are usually required to control the symptoms.
4. Targeted Therapy
If the gastric cancer is metastasized and HER2 receptor is positive, targeted therapy is used with chemotherapy to control disease progression. Approximately 20% of patients with gastric cancer metastasis may benefit from targeted therapy (e.g., Trastuzumab). Before starting targeted therapy, cancer cells must be tested for the presence of HER2 receptors. Trastuzumab is often used with chemotherapy and has fewer side effects, making it well-tolerated by most patients.
5. Immunotherapy
Current immunotherapy mainly uses immune checkpoint inhibitors to eliminate tumors by utilizing lymphocytes. Less than 5% of patients with gastric cancer express higher levels of PD-L1 or show loss of MMR enzyme, which can be targeted with immunotherapy. Immunotherapy generally has fewer side effects and can have long-lasting therapeutic effects for some patients. As immunotherapy is still evolving, it is recommended to discuss the latest information with an attending doctor.
Palliative Surgery
Palliative surgical options may include:
- Palliative partial or total gastrectomy +/- adjacent organ excision
- Endoscopic stenting
- Bypass surgery
- Feeding tube insertion
- Feeding gastrostomy
After Gastric Surgery
The stomach is an important digestive organ with functions including storing, passing, breaking down, and digesting food and drinks. After partial or total removal of the stomach, patients need to adjust their eating habits. Most patients can adapt by eating more frequently and consuming small meals each time. They should cut or chew food into small pieces before swallowing and choose easily digestible foods to reduce the workload on the digestive system, otherwise, it may cause bellyache, dizziness, and other problems such as bowel obstruction. Additionally, patients may have a reduced ability to absorb iron and vitamin B12, leading to anemia. Doctors may inject patients with vitamin B12 every one to two months or provide oral iron supplements.
Post-operative Gastric Cancer Pathological Staging
Two major staging systems are commonly used in gastric cancer:
- The tumor-node-metastasis (TNM) system, developed by the International Union Against Cancer (UICC) and the American Joint Committee on Cancer (AJCC).
- The Japanese Research Society staging, based on the location of lymph nodes with cancer in the stomach.
Prognosis
Mortality
Stomach cancer was the sixth leading cause of cancer deaths in Hong Kong. In 2018, it claimed 687 deaths, accounting for 4.7% of all cancer deaths. The crude death rates were 12.1 for males and 6.8 for females per 100,000 population of the respective sex. The age-standardised death rates of stomach cancer were 5.7 for males and 3.2 for females per 100,000 standard population.
Trend of Mortality
The age-standardised death rate for both sexes had a downward trend between 1981 and 2018.
Stomach Cancer Stage-Related Survival
The five-year survival rates for stomach cancer by stage are as follows:
- Stage IA: 71% (71% of people diagnosed with stage IA stomach cancer can survive five years or more)
- Stage IB: 57%
- Stage IIA: 46%
- Stage IIB: 33%
- Stage IIIA: 20%
- Stage IIIB: 14%
- Stage IIIC: 9%
- Stage IV: 4%
Source: National Cancer Institute, USA
Risk Factors and Prevention
Knowing the risk factors for stomach cancer is the first step. Some risk factors, such as family history, are uncontrollable. But other risk factors, such as diet and smoking tobacco products, are things you can control.
Stomach Cancer and Diet
Doctors believe the steady decline of stomach cancer cases in recent decades is largely due to changes in diet:
- Food Preservation: We now preserve food by refrigeration, rather than by salting, smoking, or pickling.
- Healthy Diet: Eating foods rich in vitamin A, vitamin C, and fiber may also lower your risk for stomach cancer.
Quitting Smoking
Quitting smoking is probably the single best decision you can make for your health. It reduces your risk for many medical problems and cancers, including cancers of the stomach, head and neck, larynx, esophagus, lung, bladder, kidney, and pancreas.
Stomach Cancer Prevention
You can reduce your risk for stomach cancer by doing the following:
- Limit or stop alcohol consumption
- Do not use tobacco products
- Avoid eating smoked and pickled foods and salted meats and fish
- Eat lots of fresh fruits and vegetables
- Eat plenty of whole grain foods, such as whole grain breads, cereals, pasta, and rice
- Maintain a healthy weight