Colorectal Cancer
Colorectal cancer includes cancers in the colon and rectum. Cancer cells can grow on the colorectal mucosa and spread to adjacent tissue and other parts of the body, causing local and systemic undesirable effects or even death. Colorectal cancer is the most common cancer in Hong Kong, accounting for 17% of all new cancer cases in 2017.
Incidence
In 2017, there were 5,635 new cases of colorectal cancer, with 3,303 cases in males and 2,332 cases in females. The male to female ratio was about 1.4 to 1. The crude incidence rates were 97.4 for males and 58.3 for females per 100,000 population of the respective sex. The age-standardised incidence rates were 50.8 for males and 31.5 for females per 100,000 standard population.
Trend of Incidence
The age-standardised incidence rate for both sexes showed an upward trend between 1983 and 2017.
Share
Cause
Inherited genetic abnormality causing colon cancer involved about 5% of the total number of cases. 95% of the colorecal cancer does not have inherited genetic abnormality. Other important factors causing colorectal cancer incluse aging, male, high fat intake, alcohol consumption, red meat, processed meat, obesity, smoking, and lack of exercise
Signs and Symptoms
Early colorectal cancers often have no symptoms. Symptoms usually appear when the cancer is in the middle or late stages. Common symptoms include:
- Anal bleeding or blood in the stool
- Change in bowel habits
- Mucus in stool
- Abdominal colic
- Tenesmus (a feeling of incomplete evacuation)
- Narrow stool
- Loose stool
- Constipation
Advanced colorectal cancer may present clinically with more severe conditions such as:
- Intestinal obstruction
- Bowel perforation and peritonitis
Share
Diagnosis
Diagnosis: Colonoscopy with tumor tissue biopsies can confirm the diagnosis of colorectal cancer. If colorectal cancer is diagnosed by Gastroenterologists / Gastroenterology physicians, patients with newly diagnosed colorectal cancers are referred to colorectal surgeons for further opinion and treatment.
Role of Colorectal Surgeons
Colorectal surgeons are the key specialists in managing patients with colorectal cancers. They oversee patient care through various stages:
- Pre-operative stage
- Operative stage
- Post-operative hospital stage
- Follow-up clinic visit stage
Stoma care is co-arranged by colorectal surgeons and stoma nurses. Even in advanced or complicated colorectal cancers, colorectal surgeons contribute to the well-being of patients and offer palliative treatment for those with advanced colorectal cancers.
Role of Clinical Oncologists
Clinical oncologists provide opinions and treatment for:
- Preoperative (neo-adjuvant) chemo-irradiation
- Postoperative adjuvant chemo-irradiation
- Palliative treatment for patients with advanced colorectal cancers
Imaging Studies
Various imaging studies are used to assess the extent and stage of colorectal cancer:
- Chest X-ray (CXR)
- Ultrasound scan
- CT scan
- MRI scan
- PET CT scan
- PET MR scan
Blood Tests
- Colon cancer tumor marker CEA (carcinoembryonic antigen)
Preoperative Staging
After reviewing all the information about the patient and the tumor status, colorectal surgeons will decide on the best surgical or non-surgical options for the colon cancer patients.
Surgery
Curative Surgery
The surgical approach in colorectal cancer depends on the characteristics of the tumor such as location, size, local invasion, lymph node metastasis, and distant or other organ/peritoneal metastasis.
- Traditional open laparotomy approach: Colectomy, anterior resection of rectum (AR), low anterior resection of rectum (LAR), total mesenteric excision of rectum (TME), abdominoperineal resection of rectum (APR).
- Mini-laparotomy: (skin incision less than 8 cm in length) + Colectomy, AR, LAR, TME, APR.
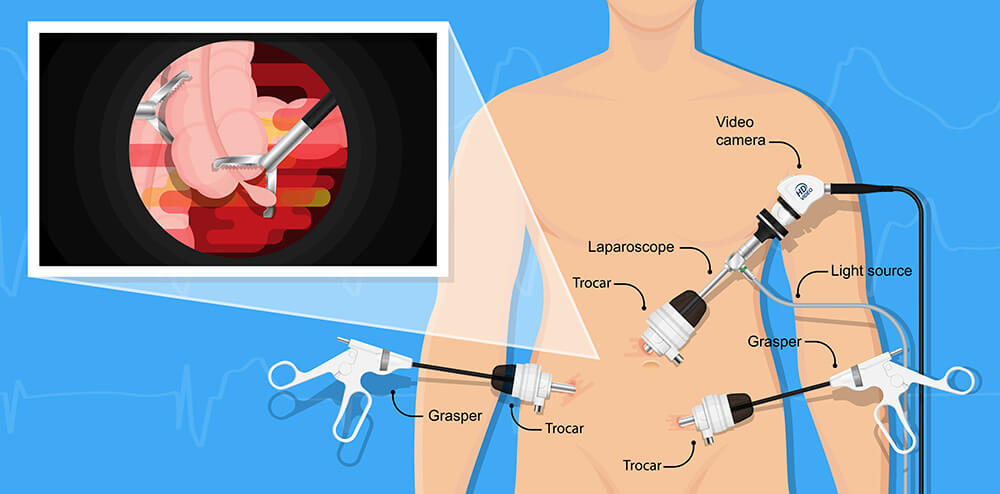
- Laparoscopic approach: + Colectomy, AR, LAR, TME, APR.
- Robotic Assisted Laparoscopic approach: + Colectomy, AR, LAR, TME, APR.
- After TME or APR, a temporary or permanent ileostomy/colostomy may be added.
For patients with Stage I, II, and III diseases, the primary treatment is surgery. For patients with Stage III disease, adjuvant chemotherapy is usually added after surgery.
Palliative Surgery
- Endoscopic (colonic/rectal) stenting
- Colectomy / anterior resection of rectum
- Bypass surgery
- Ileostomy / colostomy
Post-Operative Gastric Cancer Pathological Staging
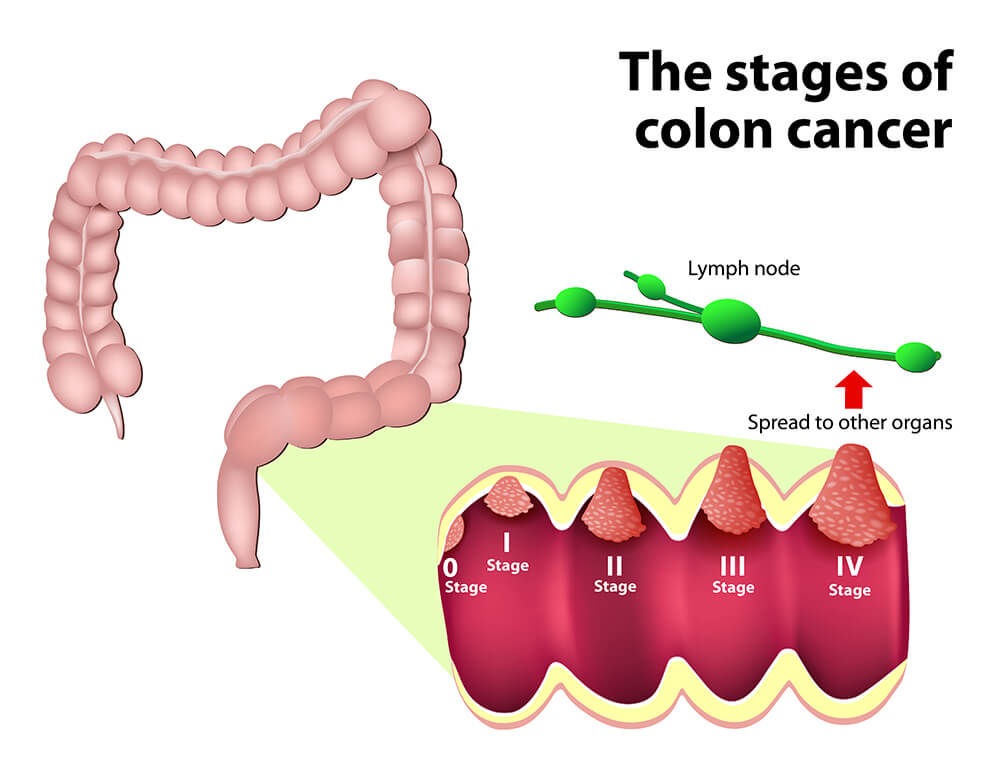
The purpose of staging cancer is to guide clinical treatment decisions and predict patient prognosis according to different colorectal cancer stages. The staging method for colorectal cancer by the United States Joint Cancer Committee (AJCC) is as follows:
- Stage 0: Carcinoma in situ, no local lymph node metastasis, no distant metastasis.
- Stage I: Tumor invasion to the submucosa or muscle layer, no local lymph node metastasis, no distant metastasis.
- Stage II: Tumors invade the muscle layer to the serosal layer or the peritoneal and rectal tissue without peritoneal coverage, without local lymph node metastasis, without distant metastasis.
- Stage III: The tumor directly invades other organs, with local lymph node metastasis, but no distant metastasis.
- Stage IV: The tumor directly invades other organs, with local lymph node metastasis and distant metastasis.
Additional Treatments
Chemotherapy
Used to treat Stage III and Stage IV colorectal cancer.
Radiotherapy
Used to treat rectal cancer to reduce pelvic recurrence and control local disease.
Target Therapy
Currently limited to patients with Stage IV metastatic colon cancer with identified targets in the cancer cells. For patients who do not benefit from chemotherapy alone, adding targeted therapy may offer some improvement.
Immunotherapy
Immunotherapy is a class of treatments that take advantage of a person’s own immune system to help kill cancer cells. There are several FDA-approved immunotherapy options for colorectal cancer, including for tumors that are microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR).
Targeted Antibodies
- Bevacizumab: A monoclonal antibody that targets the VEGF/VEGFR pathway and inhibits tumor blood vessel growth; approved for subsets of patients with advanced colorectal cancer, including as a first-line therapy.
- Cetuximab: A monoclonal antibody that targets the EGFR pathway; approved for subsets of patients with advanced, EGFR-positive colorectal cancer, including as a first-line therapy.
- Panitumumab: A monoclonal antibody that targets the EGFR pathway; approved for subsets of patients with advanced, EGFR-positive colorectal cancer.
- Ramucirumab: A monoclonal antibody that targets the VEGF/VEGFR2 pathway and inhibits tumor blood vessel growth; approved for subsets of patients with advanced colorectal cancer,including as a first-line therapy.
Checkpoint Inhibitors
- Nivolumab: A checkpoint inhibitor that targets the PD-1/PD-L1 pathway; approved for subsets of patients with advanced, MSI-H colorectal cancer.
- Pembrolizumab: A checkpoint inhibitor that targets the PD-1/PD-L1 pathway; approved for subsets of patients with advanced, MSI-H or dMMR colorectal cancer, including as a first-line therapy.
Prognosis
Mortality
Colorectal cancer is the second leading cause of cancer deaths in Hong Kong. In 2018, there were 2314 deaths caused by colorectal cancer, accounting for 15.9% of all cancer deaths. The crude death rates were 38.4 for males and 24.9 for females per 100,000 population of the respective sex. The age-standardised death rates were 18.2 for males and 11.1 for females per 100,000 standard population.
The 5-year survival rate of people with localized stage colorectal cancer is 90%. About 39% of patients are diagnosed at this early stage. If the cancer has spread to surrounding tissues or organs and/or the regional lymph nodes, the 5-year survival rate is 71%. If the cancer has spread to distant parts of the body, the 5-year survival rate is 14%. However, for patients who have just one or a few tumors that have spread from the colon or rectum to the lung or liver, surgical removal of these tumors can eliminate the cancer, which greatly improves the 5-year survival rate for these patients.
Survival rates are also available for colon cancer and rectal cancer separately:
- Colon cancer: The overall 5-year survival rate is 64%. If diagnosed at a localized stage, the survival rate is 90%. If it has spread to surrounding tissues or organs and/or the regional lymph nodes, the 5-year survival rate is 71%. If it has spread to distant parts of the body, the 5-year survival rate is 14%.
- Rectal cancer: The overall 5-year survival rate is 67%. If diagnosed at a localized stage, the survival rate is 89%. If it has spread to surrounding tissues or organs and/or the regional lymph nodes, the 5-year survival rate is 70%. If it has spread to distant parts of the body, the 5-year survival rate is 15%.
Prevention
People above 50 years old participating in regular colorectal cancer screening programs can reduce their chance of developing colorectal cancer. The stool occult blood test and colonoscopy are the most common tests for colorectal cancer screening. During colonoscopy, polypectomy or tumor biopsy can be performed. Specimens are taken out for histology examination to confirm the pathological diagnosis. Existing medical research and data are sufficient to prove that these tests can effectively reduce the incidence and mortality of colorectal cancer.
Therefore, regular colorectal cancer screening should be carried out before symptoms occur. If colorectal cancer can be detected and cured radically at the beginning of its formation, the prognosis would be much better. This reinforces the adage that prevention is better than cure.
The medical profession generally believes that adjusting diet and lifestyle can prevent colorectal cancer. The World Cancer Research Fund and the National Cancer Institute published a research report titled "Food, Nutrition, Physical Activity, and Cancer Prevention" in 2017, which includes the following recommendations for preventing colorectal cancer:
- Keep your weight in the healthy range and avoid obesity.
- Limit red meat intake (such as beef, pork, and lamb), and avoid processed meat.
- Restrict alcohol consumption.
- Increase your consumption of different types of fruits and vegetables, whole grains, and beans.
- Exercise for at least 30 minutes a day.
- Never smoke.