<Male left inguino-scrotal hernia>
Adult Inguinal Hernia
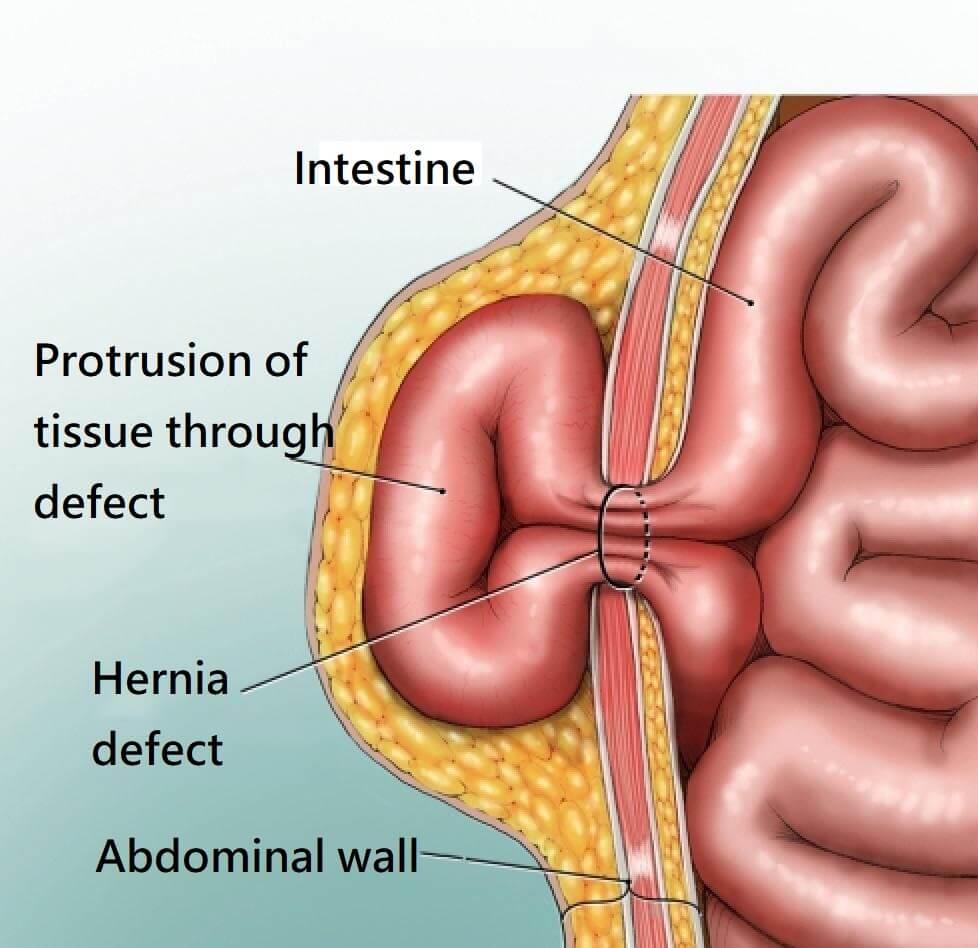
An inguinal hernia is a protrusion of abdominal-cavity contents (e.g. bowel or omentum) through the inguinal canal in the groin. Sometimes, it can extend to the scrotum in male (inguinoscrotal hernia) or to the labia majora in females.
Symptoms
Majority of the inguinal hernia patients have symptoms, e.g. (1) a soft groin swelling below the skin, (2) pain or discomfort (especially during coughing, exercise, lifting heavy objects, passing urine or during bowel opening). The symptoms often get worse throughout the day, or after standing or walking for a long period of time, and improve when lying down. A bulging at the groin or scrotum (in men) or labia majora (in women) may occur and may become larger when bearing down. Inguinal hernias occur more often on the right side than the left side. About 27% of males and 3% of females develop a groin hernia at some time in their life. About 15-20% patients have bilateral inguinal hernias.
Complications
Most inguinal hernias enlarge over time if not repaired surgically. In men, large hernias can extend to the scrotum; in women, large hernias can extend to the labia majora. Inguinal hernia can cause pain, swelling, bowel obstruction, bowel strangulation or even death. Incarcerated (Irreducible) hernia occurs if the contents of the hernia become trapped and cannot return to the abdomen. It can obstruct the bowel, leading to severe pain, nausea, vomiting, and inability to have a bowel movement or pass gas. Strangulated hernia is a dangerous stage of incarcerated hernia with the blood flow cutoff to the hernia content (ischemia), mostly small bowel and omentum. Strangulation can lead to the death of the affected small bowel tissue (gangrene), causing bowel rupture and peritonitis. If bowel ischemia, bowel gangrene, bowel rupture, and peritonitis are not treated as soon as possible, death is inevitable. Therefore, clinical diagnosis of strangulated hernia is a potentially life-threatening situation and requires immediate surgery. Signs and symptoms of a strangulated hernia include: nausea, vomiting, fever, painful groin swelling, inability to pass feces or pass gas, severe abdominal pain, tenderness upon touching, red, purple or dark discoloration of the hernia, failure of reducing the hernia etc. If you have the signs and symptoms of the strangulated hernia, please seek help immediately from the nearest emergency.
Risk factors
Risk factors for the development of an inguinal hernia include: smoking, chronic obstructive pulmonary disease, obesity, pregnancy, peritoneal dialysis, chronic liver disease, benign prostatic hypertrophy and frequent weight lifting. Hernias are partly genetic and occur more often in some families.
Diagnosis
Inguinal hernias can often be diagnosed clinically, based on signs, symptoms and physical examination. Medical imaging, e.g. X-rays, ultrasound scan, CT scan, or MRI scan, may be needed to confirm the diagnosis, assess the anatomy of the hernia or rule out other possible causes leading to hernia formation.
Indication of surgery
All hernias are generally considered as an indication for surgical repair because of the risk of pressure symptoms, bowel obstruction, or bowel ischemia. Elective surgery is preferred by all surgeons, as emergency surgery for incarceration and strangulation may carry higher risk.
Surgery
In the past, hernias were repaired by sutures and the recurrence rate was high, nearly 50%. Nowadays, using artificial mesh to fix the hernia is the standard of treatment, as artificial mesh repair can reduce the chance of recurrence to less than a few percent in ten years after surgery. Hernia artificial mesh repair may be done by:
- Traditional large incision open hernia repair surgery
- Small incision open hernia repair surgery
- (Minimal invasive) laparoscopic hernia repair surgery
Traditional large incision open hernia surgery with artificial mesh needs an incision of about 10–12 cm to fix the artificial mesh and repair the hernia.
Small incision open hernia repair surgery with artificial mesh needs an incision of about 3–5 cm to fix the artificial mesh and repair the hernia.
Minimal invasive laparoscopic hernia repair surgery with artificial mesh uses three to four small incisions (size 0.5–1 cm) to pass the instrument and videoscope to the preperitoneal area to fix the hernia with the artificial mesh.
Elective small incision open hernia repair surgery or minimal invasive laparoscopic hernia repair surgery use smaller wounds to fix the artificial mesh. The postoperative wound pain will be less, and patients can return to office work or exercise earlier. Most patients recover well and can go home one to two days after surgery. The outcome of these elective surgeries is usually very good, and the complication rate is very low.
Long-acting local anesthetic injections to the wound during surgery and postoperative oral analgesics are often used to reduce the postoperative wound pain to a minimum. Absorbable subcutaneous stitches are often used to close the hernia wounds, eliminating the need to suffer any pain during the removal of superficial stitches. Patients are usually required to keep the wound dry for 2–3 weeks. After 2–3 weeks, all the wound dressings can be removed. Patients can usually return to office work 1 to 2 weeks after surgery. Patients can often return to exercise 4 to 6 weeks after surgery.
In emergency surgery for strangulated hernia, traditional open surgery usually requires a large wound to gain access to the hernia sac, return the abdominal content to the abdomen, and fix the artificial mesh. If there is bowel obstruction or bowel perforation, major laparotomy and bowel surgery will be required to correct the problem. Emergency surgical repairs of strangulated hernias usually carry a higher complication risk, higher morbidity rate, and higher mortality rate. Patients with emergency hernia surgery often need to stay in the hospital for one to two weeks.
FAQs
Q: Can I leave my inguinal incisional hernia untreated?
A: Yes. You may choose not to treat your hernia. But you may feel pain or discomfort every time you stand or walk. As the condition worsens over time, you may face more serious complications such as intestinal ischemia, intestinal perforation, peritonitis, and even death. It is indeed unwise to leave it untreated.
Using the latest methods to treat inguinal hernia, most patients feel no pain or minor pain after surgery. Most patients can return to their favorite activities within 6 - 8 weeks. Why not seek early treatment?
Please consult your doctor for advice.
Q: Is artificial mesh repair surgery for inguinal hernia safe?
A: The latest artificial mesh repair surgeries for inguinal hernias are very safe. The operation takes about 1-2 hours, the postoperative pain is low, and the recurrence rate is low. Please consult your doctor for advice.